
Colon Polyps and Colon Cancer
Cancer of the colon is a major health problem in the United States. It ranks as a leading form of cancer, along with lung and breast cancer. Importantly, colon cancer is also one of the most curable forms of cancer. When detected early, more than 90 percent of patients can be cured. Roughly 150,000 people develop colon cancer annually and 60,000 succumb to this disease. Colonoscopy is the procedure of choice for detecting and removing growths from the colon. Colon cancer screening with colonoscopy utilizes a relatively thin, long tube with a video chip located at the tip. The system provides for high resolution color examination of colon. The instruments are equipped with working channels that allow for the passage of devices that take samples (biopsies) or remove growths (polyps). The tube is passed through the anus into the rectum and is advanced through the entire colon. A complete exam is essential and means the scope was passed into the right colon to an area called the cecum. The colon is like an inverted U in your abdominal cavity. The first area entered is the rectum, then to the left colon comprised of the sigmoid and descending colon. It continues across the upper abdomen through the transverse colon into the right colon, called the ascending colon, and into the cecum. The cecum connects to the small intestine referred to as the terminal ileum. The colon is about 6 to 8 feet long. The preparation for colonoscopy is often dreaded, but with newer formulations has been made easier. Most patients maintain a clear liquid diet the day before the test and consume a cathartic substance that forces several bowel movements until the stool appears clear. The specifics of your colonoscopy preparation will be provided by your gastroenterologist. The alternatives to colonoscopy include barium enema x-ray that must be combined with flexible sigmoidoscopy (a short scope that views the rectum and left colon) to properly view the left colon, or virtual colonoscopy. Barium enema is less senstive than colonoscopy for picking up abnormilties. Virtual colonoscopy utilizes CAT scan 3D imaging to reconstruct images of the colon. It still requires preparation and rectal tube insertion to introduce air to expand the colon. Unfortunately, it can miss small polyps (less than 0.5 centimeters) and is ususally not covered by insurance. Both barium enema and virtual colonoscopy do not allow for sampling of colon tissue. If there is an abnormality with either of these tests, then you will require colonoscopy as a definitive diagnostic test that is able to sample tissue or remove abnormal growths. No exam is perfect. Miss rates do occur with colonoscopy and have been reported to occur anywhere from 6-20 percent of the time. Routine checking of the stool for hidden or occult blood is used in colon cancer screening on an annual basis for anyone of average risk 40 years of age or above. Colonoscopy is recommended for average risk persons beginning at the age of 50. Consult with your doctor about the additional screening guidelines. Remember, any form of screening is better than none at all. If you have any alarm symptoms such as rectal bleeding, a change in your bowel pattern, abdominal pain, or unexplained weight loss, contact your doctor.
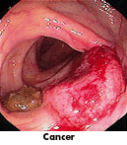
This disease begins in the cells that line the colon. There now is strong medical evidence that there is an abnormal gene for colon polyps and cancer that can be passed from parent to child. The genes within each cell are the hereditary structures that tell the cell what it should do. It is becoming increasingly clear that certain of these genes control the growth of the cells on the lining of the colon. When these controlling genes are absent, there is a tendency to grow polyps. The cells in the polyp eventually become uncontrolled and turn into cancer. Colon cancer also can develop from other conditions, such as colitis.
- What is Colon Polyp?
-
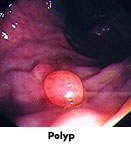
A polyp is a growth that occurs in the colon and other organs. These growths, or fleshy tumors, are shaped like a mushroom or a dome-like button, and occur on the inside lining of the colon. They may be as small as a tiny pea or larger than a plum. It is important to note that while colon polyps start out as benign tumors, some polyps, in time, become malignant. In fact, the larger the polyp, the more likely it is to contain cancer cells. In most cases, it is a polyp called an adenoma polyp that develops into colon cancer. The good news is that these growths are often dectected by colonoscopy and can be safely removed at the same time as detection.
- What Are The Risk Factors for developing Colon Polyps and Cancer?
-

Family history of polyps, cancer, and especially colon cancer.
Western civilization and diet.
Being over 40 years of age
History of breast cancer
Ulcerative Colitis
Crohn's Disease - In summary...
-
Cancer of the colon is a serious but readily detected malignancy. In addition, early detection promises a particularly high chance of survival. Most colon cancers start as polyps, which can usually be removed with an outpatient procedure. Today, much information is available to significantly reduce the risk of this disease. The essential first step involves action by the patient.
80 5th Ave. Suite 1605 New York, NY 10011
55 Montgomery St. Poughkeepsie, NY 12601
212 673 2721 845 471 1354
info@starpoli.com
55 Montgomery St. Poughkeepsie, NY 12601
212 673 2721 845 471 1354
info@starpoli.com
© 2023 AA Starpoli, MD
|Office Policies
|Privacy Policies